
Surviving Dr. G
A Patient's Fight Against Medical Gaslighting and Systemic Trauma

My birthday on November 26th brought an unexpected wave of support, with dozens of well-wishes flooding my social media feed. About a week later, I finally found time to respond, realizing just how consumed I had become by my health struggles and the relentless fight for appropriate care—I hadn’t even checked my email in a month. This moment of acknowledging those kind messages made me realize that I needed to be more open about my reality. I felt compelled to document what I was experiencing, not just for myself, but to raise awareness about the profound impact of medical gaslighting and systemic trauma. This document, Surviving Dr. G, is the result of that necessity.
August 2024. Dr. G was in a bad mood that day. I wasn’t in a great place either; my little sister had died six weeks before, I was dealing with management to remove mold from my kitchen and replace the sink and cabinets, and I had insomnia. I had a leg ulcer that had lasted for two months and red nodules on both my elbows, along with swollen feet, pronounced veins, and unusual bruising. When I was telling her about a bone pain from my hip to my knee that was similar to a growing pain, she mocked me and rolled her eyes. At one point, she clucked at me as one would do to silence a child. I mentioned to her that the hair on my arm was standing straight up and I wasn’t cold. She rolled her eyes. As a doctor, she should know this is a sign of “fight, flight, or fawn” from PTSD. When I was incarcerated in the 90s, I couldn’t fight or flee, so I learned to fawn or freeze. This is why I remember every detail of that visit. A few days later, I read her progress notes and she stated that the rash on my leg and the nodules on my elbows had resolved overnight. My lower leg was bandaged because my dermatologist had already taken a biopsy.
Self Advocacy
When I told my support group about the visit, they advised me to tell Dr. G how I felt, so I wrote her a message on the patient portal. I told her that she didn’t examine me, I felt unheard and unsafe, and I had lost some trust in her. She didn’t respond well; she got really defensive. Her response was to tell me I could get another primary care doctor if I didn’t feel my needs were being met. Her supervisor called me, and I told her that Dr. G was a great doctor and I just didn’t know what went wrong that day, and I didn’t want a new doctor. I think Dr. G might have been a bit embarrassed over the message I sent her, which was never my intent. Our next appointment was a phone call. I took responsibility and told her I was sorry, that I had probably overreacted because of my PTSD. I told her that I did have the rash and it was bandaged that day, and I had photos of my leg every few days for the two months, and I mentioned that Dr. L had done a biopsy. She got defensive again. I just wanted the right symptoms in my chart so we could figure out what was going on with me.
Escalation and Blockade
I have a complicated medical history, including autoimmune and inflammatory disorders. I also had chronic neck and spine issues that had left me hunched over. A couple of weeks after what I call “the bad appointment with Dr. G,” I had a follow-up with my allergist. When Dr.K walked in, he asked, “Why are you back? I told you weren’t allergic to anything and that the hives were probably from stress. I gave you a prescription for Prednisone for when you get hives.” I told him about my leg ulcer, and he had me take the bandage off and examined it. He immediately said that I needed to see a rheumatologist. This is when Dr. G’s passive-aggressive tactics started. She wrote the referral, but instead of using the allergist’s recommendation, she allegedly stated: “The patient insists she has an autoimmune disorder, but her inflammatory markers are not high, and she is insisting on a full workup.” She completely omitted the fact that another specialist, my allergist, had recommended the rheumatologist consultation, alongside a persistent, escalating health issue—my “spike.” Instead of coordinating care, Dr. G allegedly introduced obstacles and blocked my access to treatment, leaving me feeling isolated, panicked, and trapped.
The Confrontation
I soon noticed a disturbing entry in my chart: “REASON FOR VISIT DO NOT DISCLOSE DUE TO PRACTICE DISCRETION. CONTACT PRACTICE.” This opacity was part of the primary obstacle: the refusal to formally acknowledge my persistent symptoms. Her need to be right was her priority, making her unwilling to even consider that I could have had another autoimmune disorder. This persisted despite evidence; for instance, following a routine endoscopy, the gastroenterologist reported that I have mild Gastric Antral Vascular Ectasia (GAVE), which is an autoimmune disorder. Then, I noticed Dr. G had put Chronic Spontaneous Urticaria (CSU) in my chart. At our next appointment, I addressed this directly, which was the only time I was truly sarcastic with her. I said, “I see that I have CSU, which is also an autoimmune disorder, and one out of three people who have it have thyroid issues. My grandma had thyroid problems and took Synthroid for it. But don’t worry, I don’t think I have a thyroid issue.”
January 2025: The Ripple Effect
The impact of Dr. G’s documentation became immediately apparent at my next appointment on January 9, 2025, when I saw Nurse K. The first thing Nurse K said upon entering the room was, “You have a thyroid issue?” I responded, “No,” and handed her a list of medications and labs. She dismissed the list, saying, “Oh, it’s in the computer.” I felt like responding, “So is the fact that I don’t have a thyroid disorder, but you just chose to ask about it.” She then spent a prolonged five minutes staring intently at the computer, thoroughly reviewing my chart before proceeding. It was obvious that the sarcastic comment I had made to Dr. G about the CSU & GAVEs diagnosis, and my grandmother’s history had fundamentally changed the narrative in my file. This small interaction confirmed my fears: I was now being treated as a patient who was self-diagnosing and obsessively focused on a thyroid disorder, a perception entirely manufactured by Dr. G’s defensive reaction to my confrontation.

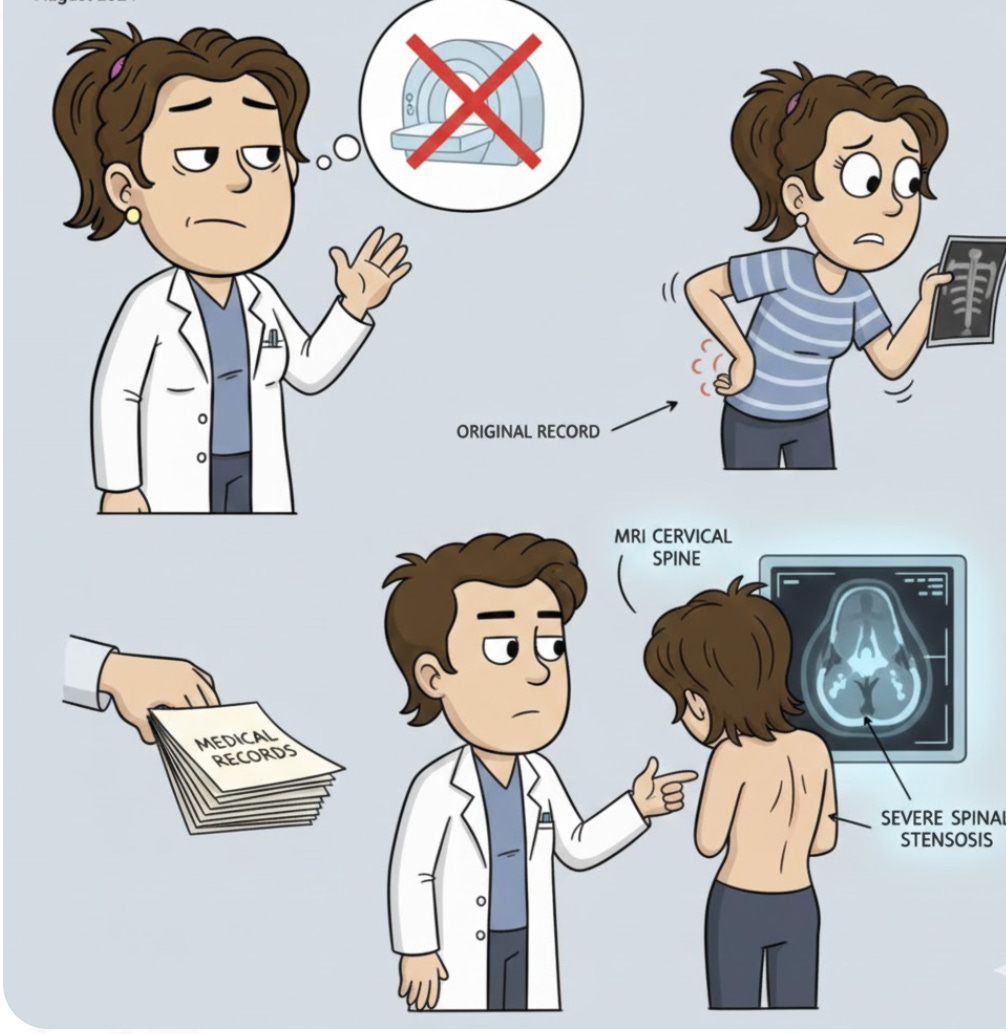
May 2025: The Blockade on the Spine
Over ten years ago, a doctor confirmed that I had multi-level degenerative disc disease with one hip higher than the other, causing occasional back issues. This time, the problem was severe, with muscles in my upper back and neck completely seized up; I had been a hunchback since November. Physical Therapy proved ineffective, and Dr. G suggested OMM (Osteopathic Manipulative Medicine). Frustrated by the lack of progress, I requested a medical records check to find the name of the doctor I had seen back in 2015. They notified Dr. G that I was requesting the records—a tactic designed to make you think you need your primary doctor’s permission to get your own records. The 2015 records showed that Dr. S had explicitly recommended: “send her to physical therapy, and if that doesn’t work, an MRI for lower lumbar would be appropriate.” Despite this expert opinion, Dr. G had previously told me an MRI was unnecessary, a sentiment echoed by the OMM doctor she had referred me to. Realizing she couldn’t deny a referral to another doctor, only the appropriate testing, I asked for a referral to see Dr. S. When I arrived for the appointment with my old and current X-rays, Dr. S examined my neck and spine and immediately ordered an MRI CERVICAL SPINE WO IV CONTRAST. The results were definitive and severe, directly contradicting Dr. G’s dismissal:
IMPRESSION: Multilevel cervical spondylosis with moderate spinal canal stenosis at C4/C5, C5/C6, and C6/C7. Multilevel uncovertebral and facet arthrosis with moderate to severe left greater than right foraminal narrowing. Severe bilateral C5/C6 foraminal narrowing.
Dr. S concluded that once my anti-inflammatory disorder is stabilized (to remove the risk of infection), I will be a candidate for a cervical epidural steroid injection and/or cervical facet procedures, based on my current symptomology consistent with cervical spondylosis with radiculopathy and cervical foraminal stenosis.
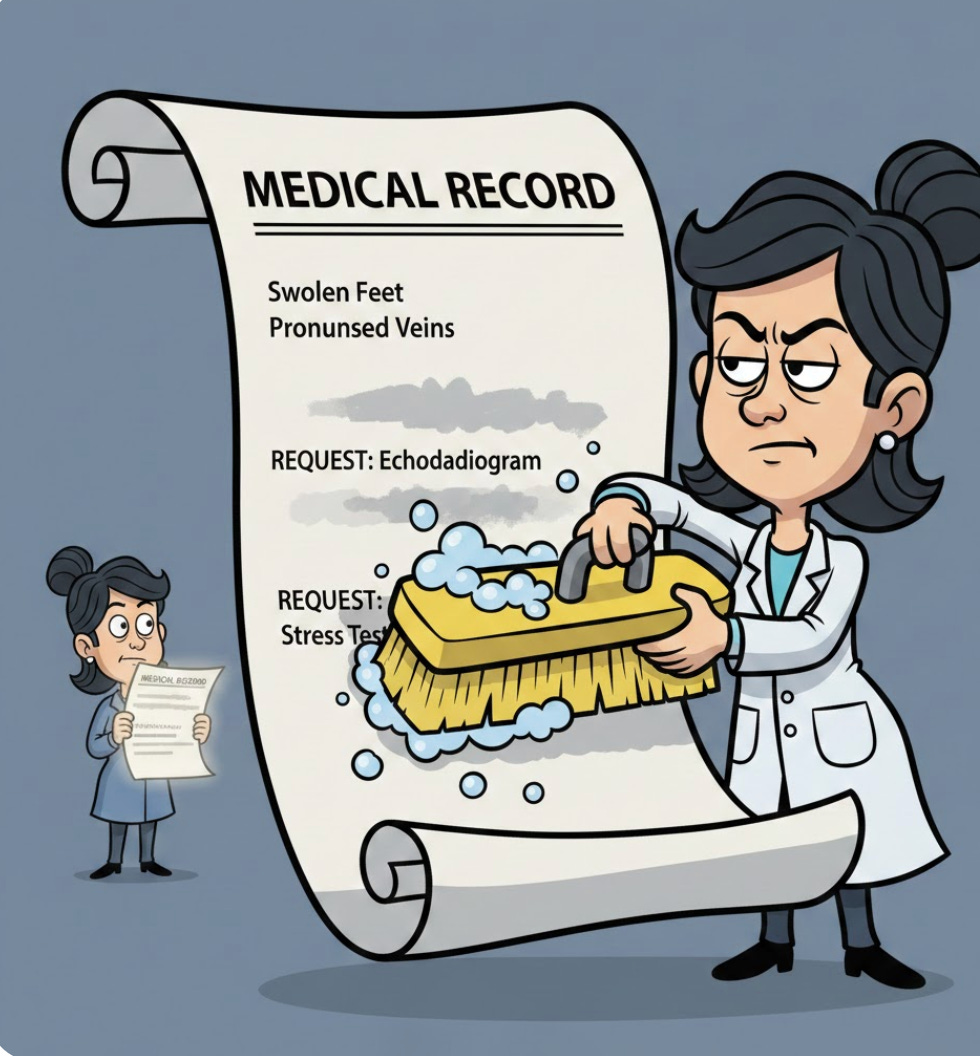
July 2025: The Evidence of Record Tampering
In June 2025, I requested two years of my medical records. On July 8, 2025, I was provided a 380-page electronic file as a PDF, a format that cannot be altered after creation. UI specifically stated that they were not to tell Dr G I was requesting my medical records as it was confidential About a week later, I had an appointment with Dr. G. After they took my shoes and socks off, I stated my feet were swollen, mentioning that my OMM doctor had suggested compression socks, and I pulled a pair from my purse. Dr. G asked, “How long have they been swollen?” and I replied, “Since August,” and we both understood this referred to the bad appointment August 2024. She walked over, listens to my heart, and says “I think I hear a heart murmur, we should order an echocardiogram.” She failed to document the suspected heart murmur in the notes for that visit. Shortly after she altered the records from the bad appointment August 2024, removing “:patient reports her feet are swollen, veins are pronounced and she has unusual bruising and requests and echocardiogram and stress test.” Altering a medical record is a felony in the state of Rhode Island.
The Systemic Toll
Between January 2025 and October 2025, the cost of this professional obstruction became staggering. In that time, I was forced into more than a dozen medical appointments across various primary care, urgent care, spinal institute, and emergency room settings, solely in the pursuit of having my symptoms acknowledged and trying to receive appropriate diagnostic testing to no avail. Concurrently, I spent three grueling months drafting a complaint to the Medical Licensing Board. I procrastinated because I was scared they wouldn’t do anything about it. The ease and confidence with which Dr. G allegedly manipulated my records suggests this is not her first time, reinforcing the belief that she operates without fear of professional accountability. Compounding this trauma is the realization that denying an elderly patient (over 60) a second opinion is considered elderly abuse and requires mandatory reporting, yet no medical professional has stepped up to report it. This reveals a systemic failure where professional self-protection overshadows patient safety and basic ethical obligations.
Conclusion: Beyond the Diagnosis
The experience of fighting Dr. G was never truly about a single diagnosis or a rheumatology referral; it was about the systemic abuse of power where the authority of one doctor was weaponized to deny appropriate care and violate trust. Having been consistently invalidated, forced to beg for tests, and had my own medical history rewritten, I now face a persistent struggle with systemic trauma and fear. The fact that medical professionals are comfortable prioritizing self-protection over mandatory reporting of potential elder abuse demonstrates a crisis in ethical accountability. This document stands as evidence that patients must constantly advocate for their own established medical reality. The fight to survive Dr. G is, ultimately, the fight to hold a broken system accountable, ensuring that no patient is ever again isolated, dismissed, and forced to choose between their health and their sanity.
A Call for Support
The emotional and physical toll of this ongoing battle has been immense, leading to significant financial hardship. Due to these chronic health issues and the relentless fight for proper care, I have been unable to work since January. If my story resonates with you and you are able to offer support, any contribution would be deeply appreciated as I continue to navigate medical supplies and daily living costs during this period of disability.
You can help support this fight for health and accountability via Cash App:
Cash App: $CoyoteRI2010
Venmo @Bella-Robinson-13
Paypal Bella@coyoteri.org. (401…525…8757)

#whatsnext